Draft version 15, December 27, 2007. Original research manuscript for publication with the first Cuban author anonymously from Cuba.
Enhancing global rural health utilizing comprehensive and electronic primary health and life care and research.
Rodolfo J. Stusser1, MD, MSc, MPH, Richard A. Dickey2, MD, FACP, FACE, Thomas E. Norris3, MD.
1 Retired of MINSAP, Scientific Pole & Havana University’s Community Polyclinics.
Correspondence to: Rodolfo J. Stusser, Freelance Research Consultant, PHC e-Research Collaboration Center, F # 256 interior apt. 2 / 11-13, Vedado, Havana 10400, Cuba. [email protected]; http://havanacenter.familydoctors.net
2 Retired of Clinical Endocrinology Department, Wake Forest University School of Medicine, Winston-Salem, NC, 27157-0001, USA. [email protected]
3 Family Medicine and Health Service Departments, University of Washington School of Medicine, Seattle, WA, 98195-6340, USA. [email protected]
Abstract (1,009 words).
Introduction
Problem: Current primary health care (PHC) providers from general practitioner (GP) or family physician (FP), and even from prescribing nurses, are too few in numbers to serve and solve well the health complexities of the rural, isolated, small, poorest villages. Research to improve PHC for the world’s poor has lagged behind that for other health issues.
Hypothesis: Integrated human development in our time must guarantee that all individuals can 1) be free to think, disagree and choose information and parties, 2) have open access to cell-phones and internet, and 3) be able to work privately and travel everywhere. They must have open access to decent and improving income, nutrition, housing, health, welfare, education, transparency, goods, services, and infrastructure. All UN defined human rights, liberties, and living levels components, provided with increasing equality, are essential. The UN Millennium Development Village Projects based on clinical economics principles is giving comprehensive primary health and life care in sub-Saharan Africa’s rural, isolated, small, poorest villages. Electronic primary health and life care (PHLC) and research with cutting-edge IT could improve this promissory approach and project.
Objective: To evaluate and enhance current global delivery of PHC service delivery and research scope and means in the rural isolated, small, poorest villages using bioethical benchmarks of modern integrated human development concepts
Methods
Research design: This is an exploratory longitudinal and cross-sectional retrospective study of results in human development and healthcare as socialism erupted in the twentieth-century. A literature review of PubMed, UN agencies and global institutions’ publications and databases was done. PHC service delivery and research scope and means were compared to other global health care levels and research issues. A twenty-country case-control study was guided by the hypothesis’ methodological principles.
Countries, indexes and years: Data for a study group of the five most closed socialist and transition countries (China, Cuba, North Korea, Russia, and Viet Nam) was compared with data for each of three country control groups: most opened capitalist and developing countries (Cyprus, Hong Kong, Singapore, South Korea, and Taiwan); much opened developed countries (France, Germany, Italy, Japan, and Spain); and most opened developed countries (Australia, Canada, Iceland, UK and USA). Comparisons used thirteen human development population indexes of secondary data [Infant mortality; longevity; adult literacy; urbanization; income; physicians; GP-wages; researchers; fixed and mobile phones; internet; civil rights and political liberties; economic freedom], mainly for three “snapshot” years (1900; 1957; 2005) were considered.
Substantive and statistical analysis: It was briefly analyzed the world human development until nowadays. Intra-national and international analyses of variance for three repeated measures of indexes by years and for four independent groups of countries were done.
Results
The conceptual and statistical framework of world human development is summarized, explaining why and how advances and delays happened.
Available data show that the underproductive socialist developing countries have tendency to stagnate and even go back, preserving only (silently rationed) physical healthcare and few other capitalist trends, but highlighting them for propaganda ideological purposes. They lived heavily subsidized by allied countries, below generalized military-paramilitary repression of individual liberties, corruption, impoverishment, hunger, malnutrition, discrimination of natives, with an unfair equity at the bottom inside a huge poverty class. Well applied modern democratic capitalism in developing countries has held in rising freedom and transparency their overall increasing and balanced trends on socioeconomic growth, nutrition, housing, income, integral health and education, and all UN defined individual rights, liberties, and living level components, along with a growing equity toward the overall freedom, wealth, and wellness levels averages in their increasing middle classes.
Other data show that PHC services receive only a small proportion of the resources for health care delivery and research.
Global rural and remote health problems of the poor require a balanced and integrated policy incorporating PHC-GP/FP services and research with development economics and behavioral change for modern healthy lifestyles and environments, using a clinical economics method. Socioeconomic development must be reintegrated with the bio-psychosocial and bio-agrarian paradigms. Spending a large majority of global research funds on research for biomedical knowledge and technology must be accompanied by investing more on PHC-GP/FP services research using a bioeconomic-psychosocial paradigm.
Poorest villages necessitate a broader model of PHLC-GP/FP services through democratic decentralized self-sustainable integral growth, with access to modern life organization and technology, nutrition, housing, health, education and other living standards. Good infant mortality and longevity results do not necessarily mean overall improvement in human integral health, wellness, and quality of life.
A proposal for improved global PHLC-GP/FP services utilizing bioeconomic-psychosocial care-delivery and research supported by IT is offered. Teams of developmental economists, physicians, prescribing nurses, psycho-sociologists, agro and IT scientists are crucial to providing care and performing research on-site, collaborating at a distance through cutting edge web based virtual clinics, and multiplying scientific capacities, supporting the local teams of GP/FP, general nurses, midwives, pharmacists, sanitary workers, health activists, teachers and village leaders.
Creation of global public-private partnerships of PHLC-GP/FP and institutes, North-South research networked virtual clinics linking rural teams in poorest and richest villages, experienced researchers, and data-mining electronic PHLC-GP/FP records from the poorest villages, can increase understanding and transform the targeted care environment. Barriers to PHLC-GP/FP services and research global net-clinics are mentioned. Limitations of the study results are stated.
Conclusions
The creation of a global human-material infrastructure of PHLC-GP/FP services and research in poorest villages of developing countries inevitably requires modern democratic decentralized capitalist growth of local individual freedom and wealth, started with financial aid to the families in the communities that should be provided by global public-private partnerships. Centralized socialist policy approaches, apparently benefiting, have inhibited modern integral human development and continue doing so.
The UN Millennium Village Project’s clinical economics approach to PHLC-GP/FP services and research is argued theoretically, logically, and factually, as the best choice available to enhance the integral health, wellness and quality of life of the world’s rural poor.
This calls for increased investment in comprehensive, balanced, and integrated clinical, health and life care and research based on a bioeconomic-psychosocial paradigm, utilizing advanced IT based networked clinics to help achieve the UN Millennium Development Goals by the 2015 goal time.
Key words: global health, rural poverty, primary care, service research, general practice, healthy lifestyle, life quality, human development, civil rights, political freedoms, socioeconomic growth, research collaboration, IT, capacity building, policy, paradigm, wellness, equity, living standards, human rights.
Article (8,447 words)
Introduction
Problem
Global primary health care and research in rural, isolated, small, poorest villages
Current primary health care (PHC) providers from fixed or mobile general practitioner (GP or family physician (FP), and even from prescribing nurses, are not enough to serve and solve well the health care and research complexities of the rural, isolated, poorest villages of around 500 inhabitants in developing countries [1-3].
Global health care and research has mainly focused on the realm of the biomedical and technological model in developed countries [4,5].
Since 1972, WONCA has promoted the improvement of PHC-GP/FP services through research. Research favoring healthy lifestyles through empowerment of the world’s rural poor nascent civil society, has lagged behind other health care levels and issues research [6].
In 1978, WHO/UNICEF in Alma-Ata, Kazakhstan (formerly one of the USSR’s fifteen republics, in Middle-Asia) promulgated the PHC “Health for All” goals: improvement of maternal, infant and immunization services, along with clean water and sanitary systems [4,7]. In the 1990s, global organizations strengthened poor countries national and global health research strategies [7-8].
By 2000, no developing nation had achieved all of “Health for All” goals due to several factors [7]. PHC-GP/FP research was scarce and mainly urban. Rural and remote PHC-GP/FP services research was not well defined in a global health research action plan developed in Bangkok, Thailand by WHO, the World Bank and others [7-8].
In 2000, a group of high and middle-income nations met in New York, USA, agreeing to give 0.7% of their GDP to developing nations with the aid of global public-private donors. The UN Millennium Development Goals and Project were established over a 1990-baseline until 2015 (panel 1) [7,9].
Panel 1
The UN-Millennium Declaration Development-Goals
Source: [9].
Global health and poverty research meetings held in Mexico, F.D., Mexico (2004) and in Bombay, India (2005) [2,10], did not adequately target rural remote PHC-GP/FP service research.
Some Spanish/US-Cuban authors wonder why so much focus in global health technology and research [4], if evidence already exists that Cuba’s socialist health care system of the past four decades has worked, and it can help achieve the Millennium Goals in the developing world [11-12].
A WHO commission recognized capitalism globalization as one of the roots of world social and health inequality [13], but not that its expanding individual freedoms, wisdom, transparency, education, health, science, wealth, and egalitarianism of altruism for the last 258 years, has decreased the historical huge inequalities caused by the generalized captivity, terror, corruption, famines, poverty, epidemics, and ignorance in the long earlier world human history [9,14-18].
Hypothesis
Cuba’s health and life care and equity in capitalism and socialism
As both experience and evidence show, rural and remote health in developing countries could be enhanced through the capitalist or the socialist way of human development [1].
Socialism erupted in 1917 in a semi-autarchic USSR little affected by the West’s economic crisis of 1929. This originated a widespread discredit of capitalism in the developing countries, and a mistaken conclusion that the democratic-market system increased the number of deprived and sick, while that dictatorial central-planning system reduced them. Then, socialism looked good, but it did not work well in any country.
This confusion was increased by massive socialist misinformation. For example, it eclipsed the fact that in 1951-52, pre-revolutionary Cuba was an advanced democratic capitalist nation with continuous immigration, increasing national sovereignty, individual civil and political freedoms, transparency, socioeconomic growth, income, nutrition, housing, transport, healthcare, welfare, education, science, art, sport, goods, services, architecture, telephone, color-TV, heliports, modern infrastructure and living standards, with tiny emigration. From 1902 to 1958, this republic had, an eight and six years military dictatorships, and about 60% of its population was ascending to the middle and even to the affluent classes through dynamic broad spectrum levels of a poverty class, decreasing in number and inequalities, compared to the most advanced nations at that time [19-21].
Cuba’s capitalist and socialist --silently rationed-- multi-tier public-private healthcare systems [19-21], as well as those of other advanced countries [9,16-18], deserve careful comparative research to help improve the world’s understanding on healthcare systems.
Modern integrated human development concept is very far from the socialist Cuba restoration by one-party military/paramilitary force of the Middle-Ages’ poorest rural villages into its modern progressing cities, surviving 49 years in subsidized and undernourished status, with six-pounds of sugar monthly per-individual, and overall discrimination against Cuban natives from military/officials and foreigners, with an increasing and unjust equity at the bottom inside a 99% poor class of its population, with constant emigration [19-21].
Human development constitutes much more than the socialist preservation from 1959 to 2007 (heavily subsidized by allied countries), highlighted for ideological propaganda purposes, of Cuba’s physical health, instruction, welfare, science, art, and sport indices trends from 1728 to 1958. Human growing, decent and balanced development must guarantee all UN defined 30 articles on human civil rights and political liberties, and 12 components of living levels [22-24]. Individuals should be free active agents of overall development in their country, rather than passive recipients of dispensed benefits, and charities from abroad. Individual liberties of information/media, thought, dissent, opportunities/choice, multi-parties, private work, traveling, cell-phones and internet [19-21], along with an increasing equity toward the overall freedom and wealth levels average within the growing middle class, are also essential. Formerly, most of the world’s people of medium and affluent classes now were poor [9,16-18].
Comprehensive primary health and life care. The UN Millennium Village Projects
Since 2004, the UN Millennium Village Projects with a primary health and life care (PHLC) strategy for families (ill socioeconomic cells) in the poorest villages of Malawi, Kenya, and dozens of other sub-Saharan African countries are working [9,25]. Each encompasses changes from health and education to agriculture and critical infrastructure with civil society support, one village at a time [9,25], thereby creating a self-sustaining socioeconomic growth surpassing the 1960s’ medicine in the community approach.
These projects use the Sachs-Ehrlich-Sanchez’s clinical economics principles and method, a combination of development economics and family medicine [9,25], within an implicit bioeconomic-psychosocial paradigm to improve the quality of health, wellness and life. It foments socioeconomic diagnosis, therapy, prevention and rehabilitation of health, life and environmental problems. An economist, GP/FP and agro-scientist comprise the project’s core team, training local mobile teams consisting of GP/FPs, prescribing and general nurses, midwives, pharmacists, sanitary workers, health activists, teachers, village leaders, etc [9,25].
Electronic primary health and life care and research with cutting-edge IT.
Medical/health informatics, telemedicine, electronic-health with cutting-edge IT based PHLC-GP/FP services, education, research, and research-collaboration are the scientific tools long-needed by GP/FP and nurses, especially in rural and remote poorest areas, to boost rural medicine/healthcare to levels comparable to that seen in urban settings.
The inclusion of these IT tools in comprehensive PHLC-GP/FP services and research from an integrated local rural, urban to a national, regional and global health and life care and research strategy can help achieve the UN Millennium Development Goals [7].
Objectives
Methods
The literature review focused on global delivery of PHC-GP/FP services and research in rural, small, isolated, poorest villages, examining papers, policies, reports, statistics from diverse sources: the PAHO (1902-), the Rockefeller-Foundation (1913-), the League of Nations (1919-1946), the Third Communist International (1919-1943), the Wellcome Trust (1936-), the World Bank, IMF, UN-Agencies (1946-) [WHO (1948-)], the Non Aligned Movement (1955-), and the US NLM’s PubMed (summaries 1950-2007), among others.
The structure, advancement and impact of urban and rural PHC-GP/FP service and research in global, regional, national health services and sciences programs were analyzed, as well as the scope, methods, means, technologies and funding sources. Findings were compared to other global health care and research levels and issues [2,7-8].
Research design
This is an exploratory longitudinal and cross-sectional retrospective study of some results in human development and healthcare as socialism erupted in a group of capitalist countries in the twentieth-century. A twenty-country case-control study using thirteen human development indices and considering three “snapshot” years (1900; 1957; 2005) was accomplished. Ten indices were selected from different UN data matrixes guided by the methodological principles of the hypothesis [7,9,22-26].
The study compared the cross-sectional international and self-controlled intra-national differences and trends of various indexes, between a socialist case group and three capitalist control groups of countries, as well as between a study period post-socialist maneuver 1958-2005 and the overall control capitalist period 1900-1957 in each group of countries, avoiding the lack of historical baseline control bias, common in current national and international human development and health studies.
Countries, indexes, years and sources
A case group 1 of five still most closed ‘socialist’ developing countries in transition to capitalism was selected and contrasted with three control groups (2, 3, 4) of five countries each, having most and more opened developing and developed capitalism, according to the ranking position by the economic freedom index in an ordered list of 157 countries worldwide [9,17-18,27-28]. They were as follows:
Thirteen human development indexes were selected by socioeconomic, civil, and political importance, data availability and reliability for the years 1900, 1957, 2005; the first two characterizing the bio-physical level/quality of health and life, while the rest characterized the economic, psychosocial, spiritual, cultural, civil, political level/quality of health and life of the people and of the physicians in the study 1958-2005 and control 1900-1957 stages. They were as follows:
Note: Authors’ adjustment and estimation of data (< # and > #) were made from multiple sources for circa 1750, 1900, 1957 and 2005, when exact data for all the population groups were not available.
Substantive and statistical analysis
The world human development was briefly and substantively analyzed historically and logically until nowadays, as well as the delivery of PHC service and research. The socialist quasi-trial (in certain way) was analyzed with the Statistical Package for Social Sciences software, version 10, 1999 (SPSS Inc., Chicago, Ill). Observed percents of improvement in each country of the first five indexes for the two periods within the three years and means ± standard deviations (s.d.) for the thirteen indexes by group of country in each year were computed. One-way analyses of variance (ANOVA) univariate F tests for repeated measures of the first five indexes measured in three years, and for the thirteen indexes by four independent groups of countries in each year were done. The first, to test overall mean differences of the indexes between the study 1957-2005 post-socialist maneuver period and the control 1900-57 period within each group of country (with Mauchly’s test of sphericity and Huynh-Feldt’s correction). The second, to test overall mean differences of the indexes between the study group 1 and control groups 2, 3, and 4 of countries in the 1900, 1957 base-line years, and 2005 post-socialist maneuver year. Post hoc range t test (with Bonferroni’s correction for multiple comparisons) of pairs of groups and of years was utilized. The significance level was of alpha = .05.
Results
World human development from 1750 to 2005 compared to 1900 and 1957 findings
Human development based in workmanship and agriculture from 11,000 years B.C. until 1750 was slow. Most human beings survived generalized famines, epidemics, aggressive environments, food and basic necessity shortages, inadequate housing, ignorance, lack of liberties, extreme poverty, despotic governments, and local and regional wars [9,17-18].
In 1750, Europe, North America, Australia, New Zealand and Japan’s income per head and living levels ratios were 1.5 or 2 to 1 in relation to India and China, and 3 or 4 to 1 in regards to more primitive zones of Africa, Asia-Oceania, Central-South America. The ratio between the smallest rich class and huge poor class was of 5 to 1 [9,17-18]. Lima, Mexico and Havana were then more opulent cities than Boston, New York and New Orleans [21].
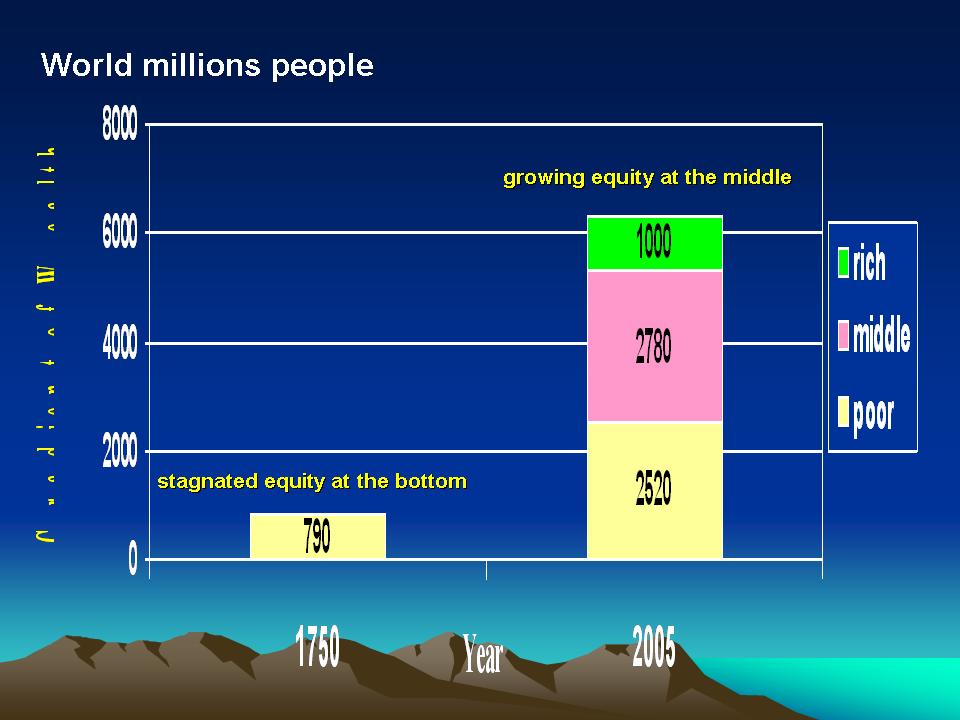
From 1750 to 2005, humanity accelerated its self-sustainable socioeconomic, civil and political local growth based on individual liberties and free-market economies. An almost global liberalization spontaneously spread industrialization, urbanization, food supplies, wealth, technological and scientific progress, democracy, egalitarianism, international trade and investment without precedent. This growth was associated with an expanding middle-class coming from the decreasing but also improving poverty class (figure 1) [9,17-18].
Figure 1
World poor class population gradient of socioeconomic advancement toward medium and affluent classes. Global results of free-market economy, open international trade and investment with self-sustainable local-development from the 1750s.
Data-source [9,16-18,35].
In a fourth of millennium of capitalism, the world’s population improved and benefited from increased nutrition, body and mental height, housing, sanitation, expanded information, liberties, rights, transparency, goods, services, and wider income distribution. It saw increased health, welfare, education, and other living levels. Urbanization enlarged twenty-four-fold, literacy improved sixteen-fold, GDP per capita increased ten-fold, longevity lengthened three-fold, and reduced infant-mortality improved by seven-fold. Most of these gains occurred mainly in the 1900s, due to a remarkable reduction in freedom, health, life and wealth inequality between the lower classes and the medium and upper classes (table 1) [9,16-21,26-35].
Table 1
World’s population ratios of improvement in some modern human development indexes. World, 1750-2005.
†: Approximated indexes for 1750 were estimated by the authors from multiple sources, excepting the GDP per-capita, which is exact by Maddison.
Data sources: [9,16-21,26-35].
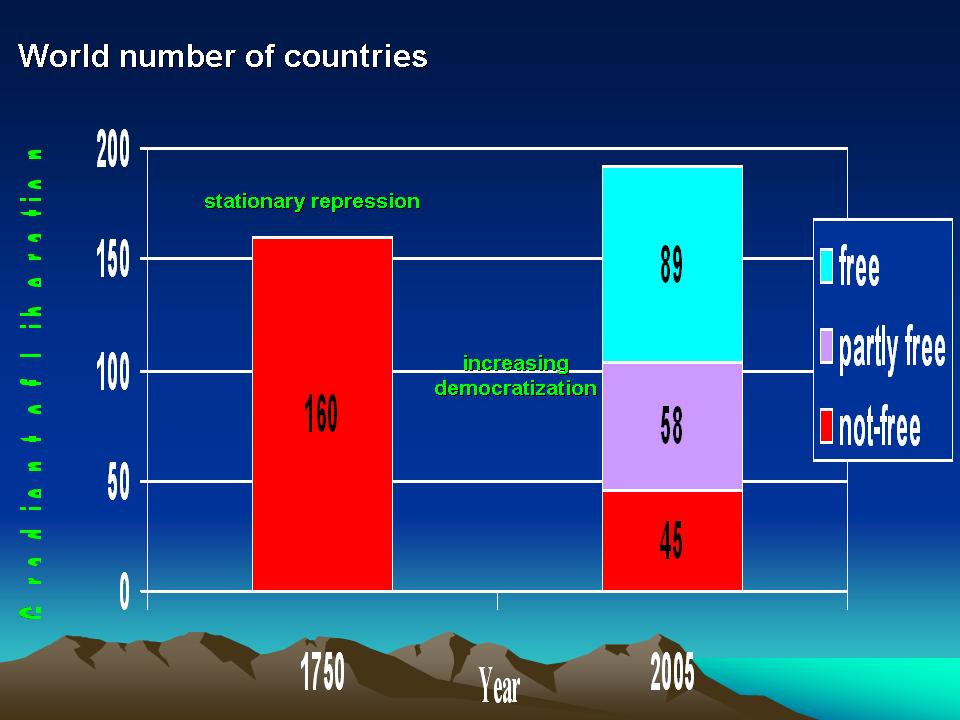
In 2005, of the world’s 6.3 billion inhabitants, about 60% have escaped from overall poverty [9], with the greatest increase of living levels occurring in those remaining in the poor class, in relation to the medium and affluent classes, which increased them, but exhibited less improvement [9,16-18]. Of great importance, nearly 50% no longer live in closed repressive systems (figures 1, 2) [9,17-18,27-28].
Figure 2
World not-free countries gradient of civil and political liberation progress toward partly-free and free individuals, peoples and countries. Global results of the human freedoms and rights and decentralized democratic and egalitarian movement from the 1750s.
Data-source: [28].
In 2005, the world’s poverty class according to World Bank definitions, consisted of 1.52 billion people in moderate poverty (daily income between US$1,00-2,00) and 1 billion-people in extreme poverty (daily income less-than US$1,00) (Figure 1) [9].
These “extreme poverty” or poorest live much as their ancestors did in 1750, surviving in the poorest villages (and later slums) of poor countries, with insufficient PHC services for infectious disease epidemics [9,16-18], and even less for the advancing non-infectious chronic disease epidemics [5].
A synchronized PHLC-GP/FP service delivery and research approach to human development as a broad expansion of all individual freedoms [24], improving lifestyles and environments from bio-psychosocial, bio-agrarian, nutritional, physiological, socioeconomic, cultural, civil, political, informatics and bioethical angles was lacking [9,16-18].
Why and how did the delay in world human development happen?
Between 1700 and 1900, the UK and three dozen developing countries (many former-colonies, such as the USA), quickly industrialized and “modernized” while most of the world’s countries lagged behind. The main causes of the lag were geographic, cultural-anthropologic and socioeconomic in nature, but lack of liberty to individual thoughts, initiatives and creation of agro-industrial scientific-technologies, along with primitive political structures, autarkic and protectionist policies, lack of commercial incentives, late colonialism and slavery, inefficient feudalist and incipient democratic capitalist systems, warlordism, corruption, and dictatorships were important too [9,16-18,24,37-39].
Liberalization, industrialization and urbanization came slowly and with difficulty to the workers of these advancing nations. In the 1900s, these continued, along with globalization of environment degradation, war, ideological subversion and terrorism. New and evolving infectious disease epidemics spread by easy and rapid transportation and tropicalization of climate threaten the health of 6.3 billion-people worldwide [9,16-18].
Russia, the fifth-largest industrialized world power in 1917 became socialist [18] and expanded in the broad USSR, suffered an exceptional internal setback and re-impoverishment of most of its people. Russia/USSR’s active external policies together with the ‘national socialism’ in Germany and fascism in Italy, retarded the spontaneous globalization of the self-sustained civil, political and socioeconomic growth of many countries contributing to re-tyrannizing and re-impoverishing the world. Soviet troops forced the institution and perpetuation of socialist dictatorships in East and Central Eurasia. Russia/USSR supported former colonies’ socialist parties and national liberation movements with massive misinformation campaigns, funds and arms. It recruited, trained and manipulated many commanders in Latin America, the Caribbean, Africa, Middle East, and Asia-Oceania [37-38].
Many newly independent parts of Africa were far richer and better developed than the nations that would later become the East-Asian tigers. For instance, in 1957, Ghana, Mozambique and Angola's GDP per-capita were equivalent to South Korea's, yet today, they are one twelfth that of South Korea's [18,30,35,39]. The external soviet-strategies stifled their development, as in many other developing countries worldwide.
Some capitalist system trends preserved and halted by the socialist system
Presented in Table 2 is the raw data matrix of the analysis. Five indexes with all the values for 1900, 1957, 2005, followed by eight indexes with values for 1957 and/or with values, ratings and ranking positions for 2004-2005, by the four groups of five countries.
Note that in the case group 1 in 1957, Russia/USSR had seen 40 years of socialism, while China, North Viet Nam, North Korea were socialist for less than eight years each, and Cuba was still capitalist until 1958. All these countries were in silent or public transition to capitalism since the 1970s.
It is important to notice that of the ten developing countries studied, capitalist Cuba was ranking in 1957, the first place, in higher physician availability; the second, in lower infant mortality, in higher literacy and urbanization; and the third position, in higher longevity, GDP per capita and phone-lines density. At that time, capitalist Cuba was better in physicians’ density than the UK, and in infant mortality than the whole control group 3 of more opened capitalist and already developed countries (table 2).
It can be seen that the five socialist developing/transition countries show a setback to IT restriction and small GDP per capita; highest civil/political rights/liberties repression, low researchers’ density (except Russia) and cheapest GP/FP-wages worldwide; while the fifteen capitalist developing/developed countries, show highest and increasing IT access, GDP per capita, rights/liberties observance, researchers’ density, and GP/FP-wages.
Table 2
Values, ratings and ranking position of human development indexes by the case and three control groups of countries. World selection, 1900, 1957, 2005.
Countries descending order is given from higher to lower ranking position by less to more economic freedom index worldwide in 2005.
Data sources: [9,16-36].
It is shown the percents of improvement in infant mortality, longevity, literacy, urbanization and GDP per capita indexes for the capitalist period 1900-57 as well as for the period coexisting capitalism with some socialist countries 1957-2005 by the respective country groups. Percent of improvement in the indexes after the post-socialist maneuver 1957-2005, were more modest in the socialist countries than in the capitalist ones, especially in GDP per capita where the change was even negative in North Korea and stationary in Cuba (tables 2, 3).
Table 3
Percent of improvement of human development indexes between the years with capitalism and with capitalism coexisting with socialist countries by the country groups.
Data source: Table 2.
Significant overall mean differences are revealed between the capitalist period 1900-57 and the period of capitalism coexisting with socialist countries 1958-2005 in infant mortality, longevity, literacy, urbanization and GDP per capita, by each respective group of countries. Non significant post-hoc mean differences were found in the socialist group in GDP per capita for both periods, even including the Russia/USSR great industrial power influencing for higher differences respect to the capitalist groups (table 4).
Table 4
Significance of differences in human development indexes between the periods with capitalism and with capitalism coexisting with socialist countries by country groups.
Data source: Table 2.
It is revealed the non significant overall mean differences in infant mortality, longevity, literacy, urbanization, GDP per capita, physicians’ availability and phone mainlines, between socialist and capitalist groups 1 and 2 of the ten developing countries in 1900 and 1957, the two base-line years of the socialist trial, proving at those years the more or less homogeneity in development of both groups, and at the same time their heterogeneity with the most advanced groups 3 and 4 of ten capitalist developed countries (table 5).
After socialism erupted in the case group 1 in 1957, significant worsening in 2005 was evident in these same indexes, except in literacy and physicians’ density, in regards to control group 2, which empowered the capitalist tendency. In group 2, the mobile phones, internet, civil rights, political liberties, and economic freedom, significantly grown to the top as in groups 3 and 4, leaving group 1 at the bottom worldwide (table 5).
The socialist in transition study group 1 had a non significant one third of the physicians availability and a non significant GP’s US$ monthly average wage even 67-fold cheaper in relation to the capitalist developing countries control 2, but in relation with both control groups 3 and 4 of capitalist developed countries, their 95-fold and 108-fold cheaper mean wages reached statistically significance (table 5).
Table 5
Significance of differences in human development indexes between the groups of socialist and capitalist developing and developed countries by each year.
Data source: Table 2.
Growth of biomedical and bio-agrarian paradigms in poorest villages.
The PHC-GP/FPs have, in the past, performed biomedical, clinical, epidemiological and health services research, research to establish healthier lifestyles, and technological clinical trials based in research centers [7-8,40].
In the 1990s and 2000s, global health research funds, although still scarce tripled and doubled in amount [7-8]. Most resources were allocated to basic, applied biomedical research done in academic or industrial laboratories and centers [41].
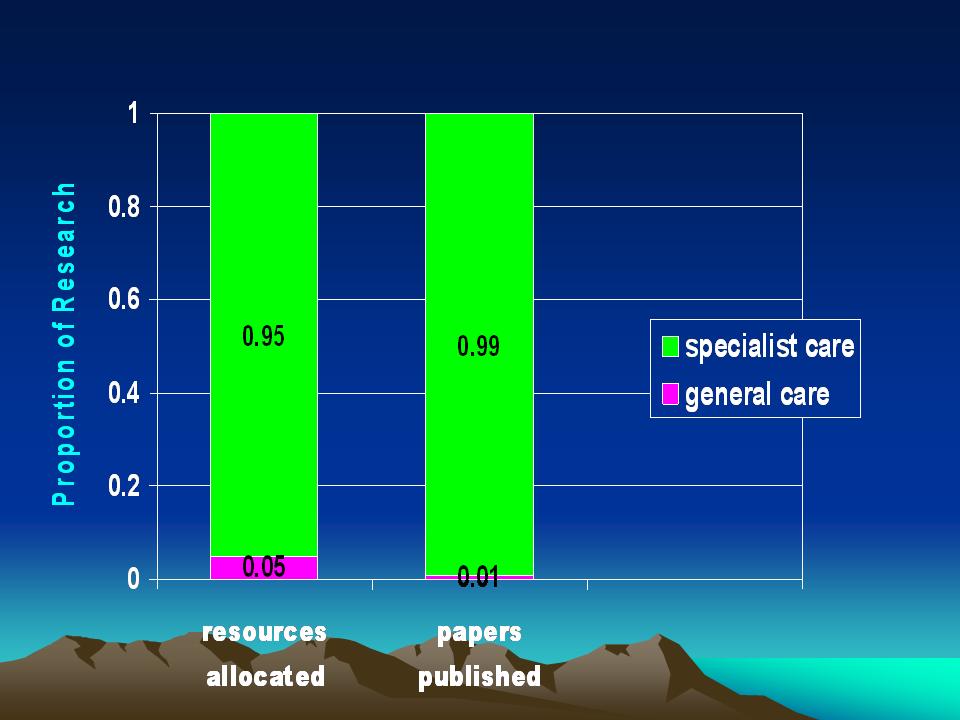
Public expenditure, not based on private sources, to support nascent PHC-GP/FP clinical and health services research in Australia, New Zealand, Holland and the UK was about $1.50 USD per-capita in 2003, while all biomedical and health research was supported at $28.00 USD per-capita (figure 3) [42].
Figure 3
Proportion of research resources allocated and papers published in general and specialty medical care. Australia, New Zealand, Holland and United Kingdom, 2002-2003.
Data-source: [42].
UN agencies, wealthy countries, World Bank, IMF and other fund donors understand the value of PHC-GP/FP service and research in favor of healthier lifestyles and environments through socioeconomic and cultural modernization of the poorest villages [43].
There has been a limited increase in capacity since the 1960s for PHC-GP/FP research, and most funds have been used for study of urban areas. The increase in PHC-GP/FP research funding is insignificant compared to the long tradition and increase in capacity (since the 1800s) for biomedical research and its industrial boom since 1945. In face of millions of full-time specialized researchers, thousand of journals and forums of exchange in traditional biomedical research; PHC-GP/FP research has few researchers, little time allocated for study, few allocated resources and limited training to allow performance of high quality research and to create forums to collectively discuss and publish results. Another problem is that the study committees that confer grants often consider PHC-GP/FP research to be of lower-quality than that from academic and industrial sites.
For example, in the mid-1980s, the basic biomedical research knowledge achieved was enough to prevent the spread of the HIV/AIDS on an economic-psychosocial basis. The 1987-2007 multi-billion US research budgets were primarily allocated to etiology, pathogenesis, molecular biology, laboratory tests, drugs, and vaccines research. This prevented allocation of funds to PHLC-GP/FP clinical and service research to change the unhealthy lifestyles and environments and end the spread of AIDS [8].
Definitive solutions to nutritional, reproductive and health problems of the poorest tropical villages, while very important [44], depend not only on bio-agrarian and biomedical sciences and technologies, availability of food, contraceptives, vaccines, tests and drugs. They also can respond to the PHLC-GP/FP services with scientific means for the study and change of behaviors, which can allow improvement in the quality of health, education, life, environment, economic security, and preservation of peace [7-8,45].
Discussion
The foundations of a global health and life care delivery and research with IT.
Capitalist and socialist human development performance from 1900 to 2005.
It would be an error to think that the solutions to the global poorest villages (and slums) problems can be found through a Marxist neo-socialism with a made up face. Just the opposite is true. The worldwide experiences in East/West Germany, North/South Korea, China/Taiwan, North/South Vietnam, and Cuba/South Florida, are there for analysis and research. Central-planning essence implies forced abolition of individual civil and political liberties and rights, massive corruption, poor socioeconomic growth, stagnation, and even setback, and unfair equity at the bottom, correspondent to outdated human development concepts.
Like Cuba, Korea had its best integrated socioeconomic, civil and political growth, including health and education, with capitalism between 1762 and 1952, largely under USA and Japan’s influences, respectively [15,19-21,39]. After 1950, the USSR and China forced both nations into fifty-year long patterns of one-man/party based repressive socialism [38], generalizing hunger (with famines), lack of individual rights, liberties, housing, transportation, mobile phones, internet access, and poorest living levels, preserving some health and education indexes’ trends to make, especially Cuba, a demonstration case for ideological propaganda purposes (tables 2-5) [15,19,21].
In the 1950s the impact of USSR rule in North Korea and Cuba inhibited the speeding up of the self-sustainable overall growth experienced in South Korea and South Florida [15,19-21]. A united, peaceful Korea might have been as powerful as Singapore (a UK Malaysian colony till 1963) or even Japan. A stable Cuba, retaining the one million political exiles who forcibly emigrated to US, might have grown more than Cyprus and be more similar to Iceland (UK and Danish colonies till 1960, 1944) [15,19-21].
Viet Nam was a very poor rural country that was divided also in North and South, militarized and left to stagnate by China and the USSR, which helped support a long and devastating war with USA [38], and its exceptional reunification under the socialist rule. Finally, after 20-years of state-based capitalism it has grown, but still has considerable hunger, corruption, lack of freedoms, rights and IT, and poorest living levels (tables 2-5).
China was the world’s technological superpower till the 1500s. Forced autarky or self-sufficiency by xenophobia, uncivilized Mongolian rule, recurrent aborted reforms attempts, and soviet socialism, fostered continued starvation and poverty. Its small but populated southeast coast with 30-years of state-based capitalism has grown, but its large northwest and central rural-communes and city workers remain poorest due in part to the fear of the communist bureaucracy that if the whole country was opened to capitalism they would lose the power [9,16-18,46].
Although the socialist countries, have all in the past manipulated socioeconomic data for propaganda, China from 1957 to 2005 reduced infant mortality seven-fold; increased longevity 62%, urbanization 173%, literacy 152%, GDP per-capita nine-fold, and GP-wage twenty-fold, surpassing the rates of same indexes improvement of North Korea, Viet Nam, and Cuba, but staying behind Asian tigers, Cyprus (tables 2-5), and others.
Had a moderate China since 1949 retained its two million political exiles who have to emigrate to Taiwan, Hong Kong, Macao and overseas since 1949, it might now be wholly advanced as the East Asian tigers (Japanese, UK colonies till 1949, 1997).
Russia, a non-standard advanced country in military and industrial development, still emerging from 75-years of soviet Leninist-Stalinist empire ideological, military and financial burdens, has partly opened its much more developed economy and its politics but has yet to see stability and more democracy (tables 2-5). A wiser Russia in 1917 would have been in every respect as developed as USA, West Germany and Japan now.
It is likely that it would have been the same with the former soviet East and Central Eurasian nations, which would have continued the rapid growth trends exhibited from 1700 to 1900. For example, Germany would have continued being the second wealthiest nation worldwide. Even former socialist East Germany needed a huge soviet subsidy, now given by West Germany. Russia/USSR and its satellites, twentieth-century largest ideological empire rich in raw resources and instructed population, unsuccessful socialist experience, must not be overlooked.
China transits toward a socioeconomic and techno-scientific superpower again.
China plans to become a socioeconomic and techno-scientific superpower in 2020 again [9,17-18,46-47]. This requires a political opening of the country. Research creativity requires individual freedom from ‘ideological walls’, from fear of criticizing authorities; to take individual initiatives and perform open-research in general production and service areas as in special institutes [17-18,40,46-47]. It demands liberated international professional exchanges through free access to travel abroad and to web-based research collaboration [48].
High-productivity research requires emancipation of native physicians, engineers, professors, scientists, technicians from the immobilizing policies of ‘egalitarianism at the bottom’ (which serve to assuage the stresses of poor socioeconomic and civil status of less qualified workers and non-workers). Professionals need all kind of spiritual and material incentives as all individual liberties and rights, and better working and living situations, similar to what the one-party bureaucrats and foreigners have lifelong.
China could accelerate the three-century liberalization movement that made the UK, France, Germany, the US, Italy, Canada, and Japan socioeconomic and techno-scientific superpowers [9,17-18], studying their advanced capitalist systems as well as capitalist Cuba [15,19-21], Cyprus, the Asian and Baltic tigers, Ireland, Chile, and others. In 2005, South Korea had the highest annual growth in patent-families (>20%), and the largest broadband penetration (260 DSL internet subscribers per thousand inhabitants) worldwide, with half of the UK’s wages (tables 2-5) [39].
China could become the rural PHLC/GP/FP’s service and research superpower with its comprehensive traditional/western medicine, first-class IT, and improved home conditions for its emigrated professionals.
Some Cuba’s health and life care socialist insights and setbacks from 1959.
Socialism produced a distorted socioeconomic and civil-political setback to the repressive and unproductive pre-capitalist monarchies. It palliates the stressing inferiority feelings of the re-generalized poorest class, subtly hiding the great inequalities with the unique party for life military/state officials. Its propaganda deviates the internal stressing starvation and penury tensions generated toward outside, blaming the US, the EU, and Japan imperialisms, uniting with faked arguments the oppressed poor masses and countries against their successful democratic and market economy policies.
Socialism faces its agricultural disasters leading to food shortages with rural forced labor camps of “educational voluntary work”, of both-sexes students, professionals and industrial-workers from the cities. Socialism based on an egalitarianism of envy [16], forces doctors, engineers, architects, scientists, technicians, qualified and productive workers into an unfair equity at the bottom, below the poverty line of the socioeconomic ladder, often even under unqualified workers and non-workers’ lowest living conditions [49].
For 45 years, socialist-Cuba has promoted, both internally and abroad, a global ideological health program by training massive numbers of indoctrinated physicians, utilizing them in fashions similar to former Soviet feldshers and Chinese barefoot doctors [49]. The covert action solidarity brigades “Inside the Deserts, Jungles and Slums” of developing nations, incite the aided poorest natives against their own medical, socioeconomic and political systems, the US, the EU, and Japan. Doctors are forced to participate in ‘Trojan Horse’ ideological subversion, with the worldwide cheapest wages, lack of information, food, housing, travels, private work, internet and mobile-phones access, rights and liberties, and decent living standards (table 2) [15,19,21,37,49].
Though is not documented with evidence yet, since the 1990s, Havana policemen coming from the Oriental-countryside are a foot-shorter than their predecessors were in the 1950s. The differences over fifty years in caloric and animal-protein consumption, height-weight and living levels have existed in socialist Cuba, between millions state employees and a few small-private farmers, and even much bigger between millions people and thousands military/state officials, famous sportsmen and artists, who used to represent a false Cuba ‘nourished, prosperous and happy’ in overseas exchanges [19,21].
Socialist Cuba’s emphasis to reduce infant-mortality at any cost (and below the US) began in 1960, when the US Program Americas’ Alliance for Progress supported the goal to halve this rate for 1970. At that time, Cuba could not reach it due to an increase in all mortality rates when the revolution socioeconomic chaos brought a first famine and misery, a four-decade decline of the elder and adult medical (and dental) quality of care and welfare, preserving better quality of care only to the infants under one year of age and pregnant women, together with heavy natality control [15,19-21]. Since the 1990s and 2000s, overall low quality of care has declined even further due to the greatest diversion of our internal resources for ideological medical activism abroad.
Germany and Japan having been devastated by the US and its allies, and rebuilt decades ago with the US support, have overcome their rancor in favor of their peoples’ prosperity. Cuba with its proximity to the US might have been more successful than the Asian, Baltic and Celtic tigers, if Havana had not been guided by Moscow (1953-1989) and Beijing (1959-1967; 1990-2007). The soviet revolution and tyranny in Cuba has no moral justification for having waged a Cold War against USA and the EU since 1953.
Current social-democratic countries such as Sweden, Norway, Denmark, and Holland had poorest villages in the distant past too, but spent centuries enriching them and their cities through democratic-capitalist growth, despite all its flaws. The UN Millennium Village Project is using the latest socioeconomic, civil, political, techno-scientific and ethical assistance to soften the adverse collateral effects of the development process of the markedly delayed capitalist growth in the poorest Sub-Saharan African countries [9,16-18,22-25].
If Africa had followed the free-market policies between 1965 and 1990 of the East Asian tigers, its average growth rate per-capita might have reached 4.3%, thus trebling personal incomes. The actual figure was 0.8% [9,35,37-38] due to non capitalist system shunts. Today, the difference in living standards between North America and Africa is 20 to 1, because North America maintained a 1.7% self-sustained economic growth rhythm for 200 years, with less population and raw materials than Africa [9,18,33,35].
Poorest villages’ health and wellness through overall self-sustainable development.
Good infant mortality, longevity, and overall human health and wellness.
In political/civil total confinement, terror, corruption, hunger, and misery, as in Cuba, lowering infant mortality (<1 yr.) to raise life expectancy at birth (highly desirable), do not necessarily mean healthier survivors with increasing equality and quality of human life and health; if this comes with native discrimination, daily indoctrination, censored media and IT, it will signify contemporary slaves unconscious of their masters, including university women prostituting with foreigners to feed and dress their children (sad tragedy). There is a global health paradox when one considers at transition countries’ data for indices such as high abortion, embryo-aspirations and sterilization rates, and life-expectancy at birth, as well as low birth-rate, infant and maternal mortalities, morbidity and mortality of transmissible diseases, etc. While these serve as indirect markers for bio-physical healthy-survival, they fail to reflect the lack of a basic, decorous, integrated, and balanced human economic, cultural, civil and political equality and quality of psycho-social and spiritual health, wellness, and life [16,18].
Under socialism the huge captive and poor population since the conception and birth survives serious shortages and diseases, reproduces and achieves longevity, but is frequently affected and disabled by new long-term chronic illnesses. Many of these illnesses are related to malnutrition, misery, confinement, lack of individual liberties, exhausting indoctrination, massive corruption, double-moral behaviors, and despair to emigrate at the cost of the life, more than to usual bio-physical and even mental illnesses. Current WHO and WONCA international disease and PHC-problems’ classifications and indexes have not yet taken these factors into account.
Today, basic human cultural, behavioral and development economics research is as urgently needed as research on the human genome was in the late 1980s, but little of the former research is yet funded [45]. If we hope to encourage persons to live with decency, honesty, responsibility, productivity, good attitudes for change, respect for races, women, natives, and other attributes of physical, mental, spiritual health, we need much more scientific research (panel 2).
Panel 2
Modern healthy-hygienic, socioeconomic, cultural, civil, and political lifestyles in poorest villages
Body
Source: [9,18].
PHLC-GP/FP research needs to be focused on these issues. Some of them, as the observance or not of each of about 60 individual civil and political liberties and rights are presented as imprecise surrogate dichotomic variables (only signed or not UN documents) in the UNDP human development index surveys [22,26], but not as real rights observed in ordinal or interval scale variables [27-28]. If these issues continue to be ignored, and the available funds continue to be invested and spent in engineering works, technological transferences, eternal subsidies and external debts waivers, without the needed PHLC-GP/FP research, they will persist, for centuries [8].
Minor differences in income and living levels still persist within developed countries. For example: In USA, survival percent ratios in elder ages (not so in young ages) in Afro-American males are still worse than Euro-American (1 to 1.24), --but even to Hindus (of Kerala) (1.17) and Chinese (1.12). In females, Afro-American ratios are also worse than Euro-American (1 to 1.5), but Chinese (1.7) are the worst. These disparities have been causally attributed to racial and sex discrimination in income, healthcare and education levels [24]. As it was observed earlier in 1750, ratios between Americans and Africans (1 to 3) at lower levels of income and living are much narrower now.
The great inequities in liberties, wealth, health, and education of the African blacks brought as slaves to USA since the 1600s-1700s, have been substantially reduced in the last 150 years, mostly in fifty years. If not, why have not Afro-Americans emigrated to Europe, India, China, Cuba or Africa, if they are free to do so? This seems to be because in any other country as in the US, the Afro-Americans would have achieved better integral health, education, and living levels, freely preserving into logical limits, most of their African ancestors’ philosophy and lifestyles, within the most relative affluence.
Afro-Americans suffer higher prevalence of hypertension, stroke, end-stage heart and renal diseases, malignancies, diabetes, obesity, homicide and unintentional injury than Euro-Americans. These produce higher mortality at mature and elder ages. It cannot be discarded that yet these Afro-American generations have not been able to fully adapt genetically to the US colder latitude and socially to the US different philosophy of life and lifestyle, so, they need more education and healthcare without coercion.
In USA the Afro-Americans have had great social difficulties, apart of biogenetics, to embrace the modern philosophy and lifestyle, even with the progressive liberties, income, health, education and social security they have had in the last 50 years. Although the sub-Saharan African blacks continue living in their original primitive tribal communities, it could be expected that they will have a longer modernization process, because most of them live still oppressed, poor, lacking healthcare and education, by their black leaders.
Balanced research on healthy social lifestyles in poorest-villages is needed.
Global health research in developing and transition nations requires additional investment and a better balance between biomedical and non biomedical research, allowing proof of the efficacy of integral progressive solutions to apparently pure biomedical problems [7-8]. Healthy social lifestyles will improve the both health and life quality with overall wellness and these in turn can drive major socioeconomic, cultural, civil and political development.
PHLC-GP/FP preventive services research capacities could interface with behavioral research centers on economic and cultural issues of healthy social lifestyles, speeding up economic growth, and reducing or eradicating AIDS, TB, malaria, parasitism, dengue fever, SARS, avian flu, social addictions, violence, corruption, and terrorism epidemics, without increased expenses in medicines and equipment [7-8].
PHLC bioeconomic-psychosocial service and research integration through IT.
Current PHC-GP/FP service delivery and research supported by IT.
In the 1990s, two scientific and technological revolutions, genomics and IT, impacted human development. Since 2004, the Gates-Foundation’s Fourteen Grand Challenges in Global Health supported mostly genomics studies in 43 research projects [4-5,7-8,44]. IT has great potential for global PHLC-GP/FP service delivery and research, but it still needs to be more adequately explored (panel 3) [7-8,48,50].
Panel 3
Potential impact of IT revolution in global primary health, wellness and life care and research.
Body
Source: [7,48,50-52].
Cognitive multilevel collaborative research has been facilitated by virtual teams of researchers in distant labs working through web-based research collaboratories (laboratories without walls). These labs arose in 1993, transmitting online text/images/voice of researchers in real time, “hands-on” identical or parallel observations, mensurations, experiments, tables, graphics, and papers, with many initiatives such as: InterMed, AIDS, Biomedical Informatics; WHO Intelligent Network, Global Projects, among many others [48,50-55].
Beginning in 2002, Practice-based Research Electronic (e)-Networks have been utilized for academic interaction, diffusion of research-results, and interface with PHC-GP/FP researchers to improve quality of care [55]. In 2004, the e-PHC Research-Network connected PHC-GPs/FPs and patients with institute-based researchers for clinical trials, providing cutting-edge technology, scientific training, and re-engineering clinical-research [57].
The five socialist transitional nations studied have lagged behind in health-IT [21,58-59], while specifically Cuba and North Korea have developed first-class military-IT applications with soviet/Russian and Chinese support. Cuba cannot do without the personal physician-patient contact and relation, due to the communist system intra- and international ideological activism with control person-to-person requirements.
Potential PHLC-GP/FP service delivery and research integration through IT.
Creating IT capabilities in rural remote poorest villages, PHLC-GP/FP practitioners and researchers could train and research in clinical economics and psycho-sociology in virtual labs, just as traditional biomedical colleagues accomplish these tasks in classic labs. This development assumes great progress in tele-medicine, surgery and health-care, distant education, and education in the use of the IT, grid and emerging cyber-infrastructure [58-59].
This PHLC-GP/FP research could be multiplied, if the virtual clinics received research funds and GP/FP assistance from well funded wealthy countries’ research programs and bioeconomic-psychosocial institutes. Global networking partnerships North-South using informatics to link the poorest with the richest village clinics and with experienced research centers could strengthen PHLC-GP/FP research capacity [7,48,58-59].
PHLC-GP/FP basic-research findings obtained from the poorest-villages’ economic-psychosocial cognitive levels could also be integrated through the internet with molecular biology results from individuals and families, and translated to applied research with the clinical bioeconomic-psychosocial approach [7-8].
Some virtual clinics could become WHO collaborating centers, coordinating research networks and consortia [7,48,58-59]. This approach could help strengthen global PHLC-GP/FP research, and aid in closing the gap between the priorities and resources assigned to this research as well as to the overall post-genome health research, thereby favoring a more comprehensive bio-psychosocial balance and electronic PHLC science.
Virtual-clinics for PHLC-GP/FP research could support data-mining of clinical bioeconomic-psychosocial electronic health records from each poorest villages, and later, at the level of the families, and much later even at the level of the individual electronic health records [7-8,48,50,57-58], helping achieve the UN-Millennium Development-Goals by 2015.
Barriers to PHLC-G/FP care delivery and research global net-clinics.
In spite of many successes achieved by these electronic tools in biomedical settings, PHLC-GP/FP researchers must still overcome challenging bioethical, methodological, logistical, interdisciplinary, privacy, sociopolitical barriers, as well as authorship protection [48,50-59].
Funding the foundations for electronic IT-based research will require global public-private-partnerships. To breakdown the technology barriers, new approaches will be needed [50-52,57-59].
New cyber-infrastructure, generations of the Internet, cell-phones and newer IT and grids will make it possible for the PHLC/GP service and research methodological arsenal to discover more comprehensive results from the human development integration of overall scientific results [58-59] from diverse cognitive levels in the remote and rural poorest villages.
Study findings limitations
The methodological limitations of this exploratory case-control observational study include the following:
Conclusions
· We present evidence that, heavily subsidized by allied countries, under-productive socialist systems in developing countries have tendency to stagnate and even go back, preserving only physical healthcare and few other social trends of capitalism, below generalized military-paramilitary repression of individual liberties, hunger, malnutrition, impoverishment, corruption, discrimination toward natives, and an unjust equity at the bottom inside a huge poorest class. Socialism have quietly rationed certain aspects of physical and mental healthcare while spending heavily on a few selected “health indexes” areas highlighted for ideological propaganda purposes. On the other hand, well-applied modern democratic capitalist systems in many developing countries, have held, in freer and wiser settings, and spurred their overall increasing and more balanced trends on socioeconomic growth, decent income, nutrition, housing, integral health and education, IT access, transparency, and improved performance on most UN defined individual rights, liberties, and living standards components, with a growing equity toward the overall freedom, wealth and wellness levels average within their increasing middle class.
· The creation of a modern global human material infrastructure of PHLC-GP/FP services and research for the rural and remote poorest villages inevitably requires modern democratic decentralized capitalist growth of local individual freedoms and wealth, participating in bioeconomic and psychosocial research, encouraging the use of technology, and providing financial aid to the families involved through global public-private partnerships. Centralized socialist policy approaches apparently benefiting, have inhibited modern integral human development and continue doing so.
· The UN Millennium Village Project’s clinical economics approach to PHLC-GP/FP service and research seems to be logically, theoretically, and factually, the best scientific way of the currently available to enhance the global rural and remote health and life of the poorest countries and regions, and many other rural villages research projects must increase to improve their health and wellness status.
· Although the genomics based biomedical and agrarian research programs for new knowledge and technologies are crucial for therapeutics and prevention of hunger and physical illnesses, they are insufficient to eradicate oppression and poverty, and to promote integral health and wellness in the poorest villages and countries, and help achieve the UN Millennium Development Goals by the 2015 goal time.
· We propose a better balanced and integrated research policy approach, with much more investments in biological science and technology based research, as well as in development economics, cultural-anthropology, behavior-politics, informatics-IT, bioethics and PHLC-GP/FP integrative research programs, guided by a bioeconomic-psychosocial paradigm.
· We propose employing the clinical economics method to diagnose and treat poorest village development problems, while simultaneously investigating the human environment biological nature as well as the behavior, culture, economics of families and individuals, promoting modern and healthy social lifestyles and environments, and resulting in improvement in their quality of health and life.
· Rural and remote PHLC-GP/FP service and research, short of well qualified physicians, would be strengthened by use of electronic care and research collaboration internet-based in mobile clinical teams, increasing quanti-qualitatively national and global capacities. Flooding developing countries with cheapest ideological physician activists who used to partially substitute nurses, midwives, pharmacists, and sanitary workers, indispensable to develop a local health system is a costly solution for their medium and long-term integral health and life care.
· This PHLC-GP/FP approach and North-South/South-South virtual research clinics would encourage the disadvantaged research programs to link isolated rural PHLC-GP/FP clinics of poorest villages to the richest villages and countries with experienced researchers nationally and globally.
· Clinical behavior, cultural and economic research results at the poorest villages could interface through electronic networks with post-genome biomedical, agrarian, and other high-technology research results of established research centers through a more comprehensive and electronic PHLC-science integration program.
· The collaboration and integration of bioeconomic and psychosocial care and research programs results would increase their quality, cost-benefits and impacts over the global health, life and overall wellness of the rural and remote poorest populations. Increased support by the UN, high and middle income nations and other global donors could help achieve the UN Millennium Development Goals.
· After a study of these proposals one might surmise that even more may be learned by use of a larger random stratified sample of countries and more key indexes, integrating all types of PHLC-GP/FP scientific models, paradigms, strategies, methods, biotechnologies, IT, other technologies, engineering, and decentralized local economic assistance --including micro-loans for the promotion of small businesses.
Competing interests
The authors declare that they have no financial conflicts or other conflicts of interests regarding the ideas expressed; and are only encouraging deep meditation and research, not suggesting prescriptions. No organization encouraged or financed this study. It expresses the authors’ own criteria on an international basis and does not represent criteria or policies from health or academic authorities of any particular country.
Acknowledgements
The authors acknowledge the architect Maria D. Espinosa for her valuable conceptual discussions and continued support, and psychologist Vivian Stusser for her assistance with its redaction.
References
1. Geyman JP, Norris TE, Hart LG (Eds). Textbook of rural medicine, 1st edn. New York: McGraw-Hill Professional, 2001.
2. Global Forum for Health Research. Global forum update on research for health. I. Poverty, equity, and health research. II. Combating disease and promoting health. Geneva: GFHR-Secretariat Pro-Book, 2005-2006. Available: http://www.globalforumhealth.org/ (Accessed 25 December 2007).
3. WHO. The health of the people: the African regional health report. 2007. Available: http://whqlibdoc.who.int/afro/2006/9290231033_eng.pdf (Accessed 25 December 2007).
4. Cohen J. The new world of global health. Science 2006; 311: 162-167.
5. The Economist. The maladies of affluence. The poor world is getting the rich world's diseases. The Economist (Online) 2007 (9 August). http://www.economist.com/world/international/displaystory.cfm?story_id=9616897 (Accessed 25 December 2007).
6. Rosser WW, van Weel C, eds. Improving health globally and the need for primary care research: Report of WONCA Kingston-conference. Annals of Family Medicine 2004; 2: S1-S64. Available: http://www.annfammed.org/content/vol2/suppl_2/ (Accessed 25 December 2007).
7. Stusser RJ, Dickey RA, Rodríguez A. Primary care and family medicine e-health research to help achieve the millennium-development-goals. Annals of Family Medicine (Online) 2004 (5 June). http://www.annfammed.org/cgi/eletters/2/suppl_2/s2#800 (Accessed 25 December 2007).
8. Stusser RJ. Post-Bangkok and pre-Mexico reflections. In: Council on Health Research for Development: Voices from Bangkok to Mexico. Geneva: COHRED; 2004. Available: http://cohred.org/cohred/content/781.pdf (Accessed 25 December 2007).
9. Sachs JD. The end of poverty. Economic possibilities for our time, 1st edn. New York: Penguin Press, 2005.
10. WHO. World report on knowledge for better health. Geneva: RPC-WHO; 2004. Available: http://www.who.int/entity/rpc/meetings/en/world_report_on_knowledge_for_better_health.pdf (Accessed 25 December 2007).
11. Franco M, Cooper R, Ordunez P. Making sure public health policies work. Science 2006; 311: 1098.
12. Franco M, Kennelly JF, Cooper RS, Ordunez-Garcia P. [Health in Cuba and the millennium-development-goals]. Revista Panamericana de Salud Publica 2007; 21: 239-250. Available: http://journal.paho.org/uploads/1182780305.pdf (Accessed 25 December 2007).
13. WHO Commission on Social Determinants of Health. Interim statement. Achieving health equity: from root causes to fair outcomes. 2007. (accessed 3 Oct 2007). http://www.who.int/social_determinants/resources/csdh_media/csdh_interim_statement_07.pdf
14. Charlton BC. Capitalism is a force for good. British Medical Journal 2007;335: 628-629. (accessed 3 Oct 2007). http://www.bmj.com/cgi/content/full/335/7621/628-b
15. Anonymous Cuban professional. Achieving health equity with more liberty, wealth, and ethics. British Medical Journal 2007 (Oct 5). Available: http://www.bmj.com/cgi/eletters/335/7621/628-b#177601 (Accessed 25 December 2007).
16. Engelhardt HT. The foundation of bioethics, 2nd edn. New York: Oxford University Press, Inc., 1996.
17. Fogel RW. The escape from hunger and premature death, 1700–2100: Europe, America, and the third world, 1st edn. New York: Cambridge University Press, 2004.
18. Landes DS. The wealth and poverty of nations: why some are so rich and some so poor? 1st edn. New York: WW Norton & Co., Inc., 1999.
19. Anon. Cuba's delayed transition needs. Lancet 2006; 368: 1323. Available: http://www.thelancet.com/journals/lancet/article/PIIS0140673606695445/fulltext (Accessed 25 December 2007).
20. McGuire JW, Frankel LM. Dimensions and determinants of mortality decline in pre-revolutionary Cuba. Harvard Center for Population and Development Studies, Working Paper Series. vol. 14 no. 6. Cambridge, MA, 2004. Available: http://www.globalhealth.harvard.edu/hcpds/wpweb/McGuire_wp1406.pdf (Accessed 25 December 2007). Finally: McGuire JW, Frankel LB. Mortality Decline in Cuba, 1900-1959: Patterns, Comparisons, and Causes. Latin American Research Review 2005:40(2):83-116. http://muse.jhu.edu/login?uri=/journals/latin_american_research_review/v040/40.2mcguire.html (Accessed 7 May 2009)
21. Stusser RJ. Progress on health care, research, education policies and systems in Cuba from 1492 to 2003. Next 10-20 years scenarios, Digest of lectures given to US people to people professional ambassadors program. Havana (Online) 2000-2003. Available: http://havanaptpclub.fortunecity.com/conference.htm (Accessed 25 December 2007).
22. UN. Universal declaration of human rights. New York: UN Publ; 1948. Available: http://www.un.org/Overview/rights.html (Accessed 25 December 2007).
23. UN. Report on international definition and measurement of standards and levels of living. New York: UN Publ; 1954.
24. Sen A. Development as freedom. 1st edn. New York: Alfred A. Knopf, Inc, 1999.
25. Earth Institute at Columbia University/UNDP. The millennium village project, 2007. Available: http://www.earthinstitute.columbia.edu/sections/view/9 (www.millenniumvillages.org) (Accessed 25 December 2007).
26. UNDP. Human-development-index tables, 1990-2007. Available: http://hdr.undp.org/hdr2006/pdfs/report/HDR_2006_Tables.pdf (Accessed 25 December 2007).
27. Heritage Foundation. Indexes of economic freedom. WCAS, 2007. Available: http://www.heritage.org/research/features/index/countries.cfm (Accessed 25 December 2007).
28. Freedom House. Freedom in the world 2006. Annual global survey of political-rights and civil-liberties, 2006. Available: http://www.freedomhouse.org/uploads/pdf/charts2006.pdf (Accessed 25 December 2007).
29. UN. Demographic yearbook 1957-1967. New York: UN Publ; 1958-1968.
30. UN. Statistical yearbook 1957-1967. New York: UN Publ; 1958-1968.
31. University of California-Berkeley/Max Planck’s Institute for Demography Research. Human mortality and life tables databases, 2007. Available: http://www.mortality.org ; http://www.lifetable.de (Accessed 25 December 2007).
32. UNESCO. Progress of literacy in various countries; World illiteracy at mid-century. Monographs on fundamental education VI, XI. Paris: UNESCO Publ; 1953, 1957. Available: http://unesdoc.unesco.org/images/0000/000029/002930eo.pdf (Accessed 25 December 2007).
33. UN. World population prospects: The 2005 revision, 2007. Available: http://esa.un.org/unpp (Accessed 25 December 2007).
34. UNICEF. Annual report statistical tables, 1990-2007. http://www.unicef.org/sowc07/docs/sowc07_tables.pdf (Accessed 25 December 2007).
35. Groningen Growth Development Center. Total economy database; Angus Maddison historical statistics database, 2007. Available: http://www.ggdc.net/ (Accessed 25 December 2007).
36. US-National Bureau of Economic Research. Occupational wages around the world; International labor organization, 2007. Available: http://www.nber.org/oww/ ; http://laborsta.ilo.org (Accessed 25 December 2007).
37. Anon. UN and WHO leaders could welcome a bioeconomic-psychosocial paradigm. British Medical Journal (Online) 2006 (Nov 15). Available: http://www.bmj.com/cgi/eletters/333/7576/1015#149265 (Accessed 25 December 2007).
38. Andrew C, Mitrokhin V. The world was going our way. The KGB and the battle for the third world, 1st edn. New York: Basic Books, 2005.
39. Webb M. South Korea: Mass innovation comes of age. In: Demos. The Atlas of Ideas. 2007. Available: http://www.demos.co.uk/files/Korea_Final.pdf (Accessed 25 December 2007).
40. Stusser RJ. Reflection on the scientific method in medicine. In: Medical sciences. Encyclopedia of Life Support Systems. Oxford, UK: UNESCO, EOLSS-Publishers, 2006. Available: http://www.eolss.net (Accessed 25 December 2007).
41. UK-Department of Health. Best research for best health: a new national health research strategy in England. London: UK-Department of Health; 2006. Available: http://www.dh.gov.uk/assetRoot/04/12/71/52/04127152.pdf (Accessed 25 December 2007).
42. McAvoy BR. Primary care research—what in the world is going on? Medical Journal of Australia 2005; 183: 110-112. Available: http://www.mja.com.au/public/issues/183_02_180705/mca10267_fm.html (Accessed 25 December 2007).
43. Lam CLK. The 21st century: the age of family medicine research? Annals of Family Medicine 2004; 2: S50-54S. Available: http://www.annfammed.org/cgi/content/full/2/3/282 (Accessed 25 December 2007).
44. Juma C, Yee-Cheong L. Millennium project. Reinventing global health: the role of science, technology, and innovation. Lancet 2005; 365: 1105-1107.
45. Stusser RJ. The unity of human being health needs a program of human health, development, medicine, and behavior projects, to integrate with the genome project. Project presented in 4th Forum/IC2000, Oct. 10-13; Bangkok; (Online) 2000. Available: http://rational.fortunecity.com/integration2.html (Accessed 25 December 2007).
46. Wilsdom J, Keeley J. China: The next science superpower. In: Demos. The Atlas of Ideas. 2007. Available: http://www.demos.co.uk/files/China_Final.pdf (Accessed 25 December 2007).
47. The Lancet. Reforming research in China. The Lancet 2007; 369: 880. Available: http://www.thelancet.com/journals/lancet/article/PIIS014067360760419X/fulltext (Accessed 25 December 2007).
48. Stusser RJ, Dickey RA, Kriel RL, Krach LE. How the internet could help Cuba more in health research. British Medical Journal 2004; 328:1209. Available: http://www.bmj.com/cgi/content/full/328/7449/1209 (Accessed 25 December 2007).
49. Anonymous Cuban professional. Poverty, emigration, government, development, and equity. Annals of Family Medicine (Online) 2007 (3 December). Available: http://www.annfammed.org/cgi/eletters/5/6/486#7388 (Accessed 25 December 2007).
50. Norris TE, Goldberg HI, Fuller S, Tarczy-Hornoch P. Editors. Informatics in primary care, 1st edn. New York: Springer Verlag, 2002.
51. Teasley S, Wolinsky S. Scientific collaborations at a distance. Science 2001; 292: 2254-2255.
52. National Center for Research Resources. Report of meeting on data and collaboratories in the biomedical research community. 2002 Sep 16-18; Arlington, Virginia. Bethesda: NIH-NCRR; 2002. Available: http://www.crew.umich.edu/publications/02-01.doc (Accessed 25 December 2007).
53. Shortliffe EH, Patel VL, Cimino JJ, Barnett GO, Greenes RA. A study of collaboration among medical informatics research laboratories. Artificial Intelligence in Medicine 1998; 12: 97-123.
54. Brauer G. Implementation of the research agenda system. Intelligent research networks (IRENEs). In: A research policy agenda for science and technology to support global health development in the 21st-century. Geneva: RPS-WHO; 1997; 106-115.
55. Collaboratory for Research on Global Projects (CRGP). About CRGP. Available: http://crgp.stanford.edu/ (Accessed 25 December 2007).
56. US-Agency for Health Research and Quality. Primary Care Practice-based Research e-Networks (PBRNs) Initiative. Available: http://www.ahrq.gov/research/pbrn/pbrninit.htm (Accessed 25 December 2007).
57. Electronic Primary Care Research Network (ePCRN). Join the future of practice based research. Available: http://www.epcrn.org/ (Accessed 25 December 2007).
58. Stusser R, Rodriguez A, Albert M, Enriquez J. [e-Network and Center for Online Research-Collaboration for Primary-Health-Care. Project submitted to the Public-Health-Ministry and Informatics-Sciences-University]. (Online) 2004-2005. Available: http://advancedgroup.fortunecity.com/initiativenhsresearch.htm (Accessed 25 December 2007).
59. Stusser RJ, Albert MJ, Rodriguez A, Echevarría S, Gonzalez RI, Cuadot A. [Vedado Project: electronic-health in primary health care. Design and initial results.] Revista Cubana de Medicina General Integral 22: (4). (Online) 2006. Available: http://bvs.sld.cu/revistas/mgi/vol22_4_06/mgi14406.htm (Accessed 25 December 2007).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}